



The CDC’s Flip-Flop Strategy: Vaccinating Kids to Protect Seniors—and Vice Versa
'So they're literally saying, give a medical treatment to someone who doesn't need it so they could maybe benefit someone who they think would'


In a recent review of an old CBS report by investigative correspondent Sharyl Attkisson, which she herself unearthed late last year, podcaster Jimmy Dore noted that the CDC repeated its flu vaccine strategy during COVID-19: When the shot fails the most at-risk group—seniors—shift the focus to vaccinating children under the guise of protecting adults. A similar approach had also been used with pertussis, promoting vaccination of older children and adults around newborns to protect infants from infection.
Flu Shots Don’t Protect Seniors From Dying—but Don’t Tell Anyone
Attkisson recently posted the transcript and a link to the 2006 CBS report on the flu vaccine. The report had been taken off the internet and memory-holed. Why? It showed that the flu vaccine does not protect seniors, the segment of the population most likely to die from the flu and its complications.
During her news report, Attkisson presented a graph (screenshot below) showing what health officials expected: as flu vaccination rates among seniors climbed from 15% in 1980 to 65% in 2001, deaths should have decreased.

But that’s not what happened. The death rate continued to rise.

Dr. Walter Orenstein, former head of the CDC’s immunization program, recognized the problem publicly.
Dr. Walter Orenstein was among the first to notice the problem when he headed up the Centers for Disease Control’s national immunization program. He says it’s now become a consensus among public health experts.
Dr. Orenstein: “What is absolutely clear is that there is still a substantial burden of deaths and hospitalizations out there that has not been prevented through the present strategy.”
The National Institutes of Health (NIH) conducted a study to verify Orenstein’s conclusion. But no matter how they analyzed the data, they kept arriving at the same result: The flu vaccine was not preventing deaths.
An important and definitive “mainstream” government study done nearly a decade ago got little attention because the science came down on the wrong side. It found that after decades and billions of dollars spent promoting flu shots for the elderly, the mass vaccination program did not result in saving lives. In fact, the death rate among the elderly increased substantially.
But when they finished, no matter how they crunched the numbers, the data kept telling the same story: flu shots were of no benefit to the elderly. Quite the opposite. The death rate had increased markedly since widespread flu vaccination among older Americans. The scientists finally had to acknowledge that decades of public health thought had been mistaken.
Studies in other countries that followed the one by the NIH came to the same conclusion, she noted, linking to an Italian study. From the study’s abstract:
After the late 1980s, no decline in age-adjusted excess mortality was associated with increasing influenza vaccination distribution primarily targeted for the elderly. These findings suggest that either the vaccine failed to protect the elderly against mortality (possibly due to immune senescence), and/or the vaccination efforts did not adequately target the frailest elderly. As in the US, our study challenges current strategies to best protect the elderly against mortality, warranting the need for better controlled trials with alternative vaccination strategies. (Emphasis added.)
The NIH barred Attkisson from interviewing the study’s lead author. But she traveled to Boston to speak with Dr. Tom Reichert, the only co-author not employed by the agency.
Dr. Reichert: “We realized we had incendiary material.”
Attkisson: Dr. Reichert said they thought their study would prove vaccinations helped.
Dr. Reichert: “We were trying to do something mainstream. That’s for sure.”
Attkisson: “Were you surprised?”
Dr. Reichert: “Astonished.”
Attkisson: “Did you check the data a couple of times to make sure?”
Dr. Reichert: “Well, even more than that. We’ve looked at other countries now and the same is true.”
As Attkisson noted, this meant billions of taxpayer dollars were wasted on ineffective flu shots for seniors.
That [international] study, soon to be published, finds the same poor results in Australia, France, Canada and the UK. And other new research stokes the idea that decades of promoting flu shots in seniors, and the billions spent, haven’t had the desired result.
How did the CDC respond? Instead of admitting failure, they doubled down, looking for new strategies. Attkisson quoted Dr. Ann Schuchat, head of national immunization for the CDC, who said they are discussing the matter.
There’s an active dialogue about how we can do better to prevent influenza and its complications in the elderly.
In the meantime, Attkisson reported, the CDC still tells seniors to get flu shots—hoping they might reduce severity or prevent complications. The CDC may also look for a “roundabout way” to protect seniors—by vaccinating children.
But watch for CDC to likely shift in the near future more toward protecting the elderly in a roundabout way by vaccinating more children and others around them who could give them the flu.
She concluded with the following:
(Note: the government quickly followed this news with a recommendation to vaccinate children and infants for flu.)
Jimmy Dore: Vaccinating the Healthy to Protect the Vulnerable is 'Chilling'
Jimmy Dore was joined by Kurt Metzger for his review of Attkisson’s report. They were particularly upset with the CDC’s call to vaccinate children who don’t need a flu shot, noting that the same thing has just happened all over again.
Dore: (at 3:36):
So they're doing that. So they were saying that back in 2006: 'Hey, give the flu shot to people who aren't at risk from the flu so you can protect someone who is.. . . .
So they're literally saying, give a medical treatment to someone who doesn't need it so they could maybe benefit someone who they think would—even though their own study shows …
Metzger:
Hey, it's worth experimenting with though, right? Hey, it's worth the human experimentation. Twenty years ago, I'm wondering—if they were doing this 20 years ago—how they managed to make the same mistake again. That's a little bit hard to believe it's a mistake.
Dore (at 4:33) states that the CDC’s intent to vaccinate children ostensibly to protect the elderly is the most alarming part of her report:
To me, this is the part that is the most chilling
He then proceeds to replay that segment of the report:
Watch for the CDC to likely shift in the near future more toward protecting the elderly in a roundabout way by vaccinating more children and others around them who could give them the flu.
Dore (at 5:21) emphasizes that reports like this are why they want censorship:
I mean, this is why they want to have censorship on social media—because you find stuff like this.
Dore relates it directly to strategies employed during COVID-19 (at 7:53):
And that's the same thing they've told you during COVID. They're still recommending it for pregnant women and kids because it's 'safe and effective,' even though there are no long-term studies. Don't worry about that—shut up.
Metzger:
Well, I think there are [long-term studies], because I think RFK Jr. was quoting the long-term studies …
When a Strategy Doesn’t Work, Expand the Campaign
This strategy isn’t unique to the flu or COVID-19. The CDC also attempted a similar approach with pertussis cocooning—vaccinating those around newborns to protect them from whooping cough. However, studies later showed cocooning was ineffective at preventing infant pertussis deaths, yet the strategy was widely promoted before being quietly abandoned.
The Immunization Action Coalition, in partnership with the CDC, held a conference call in May 2012 entitled: “Preventing pertussis in infants: ACIP's Tdap cocooning recommendations” to review the cocooning initiative instituted six years earlier and the results, and to agree on recommendations going forward. ACIP is the CDC’s Advisory Committee on Immunization Practices. The following are several slides from the presentation:
Slide 5: The source of pertussis transmission was unknown in over 50 percent of the cases. Of the ones where the sources were identified, 75 to 83 percent were family members and those close to the family.
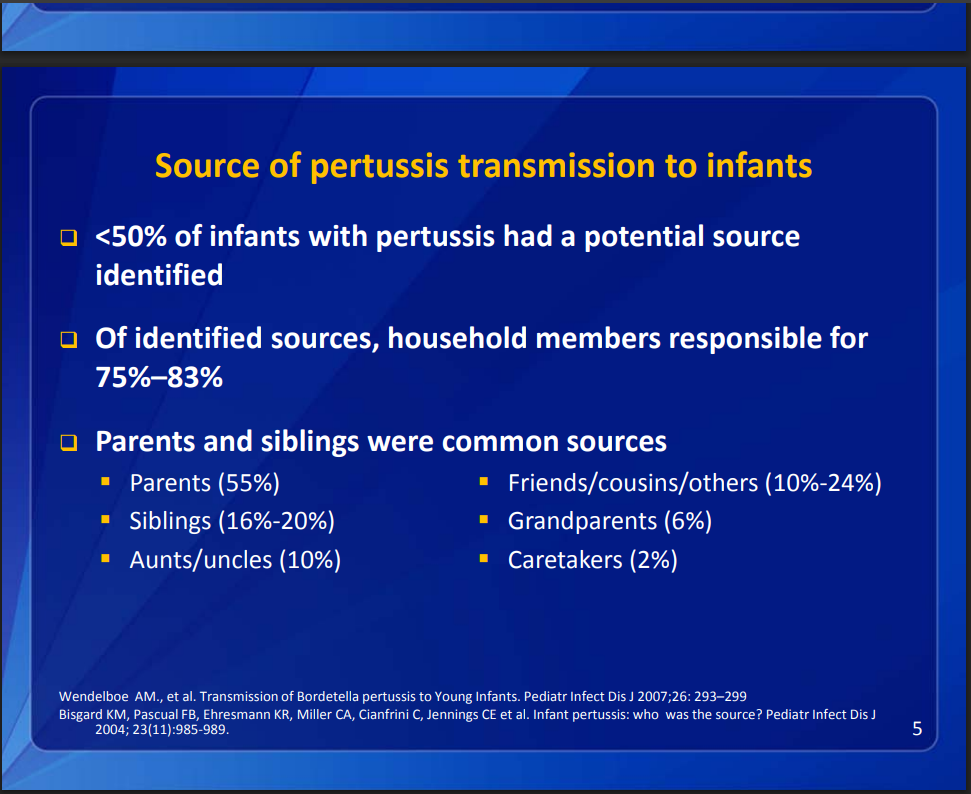
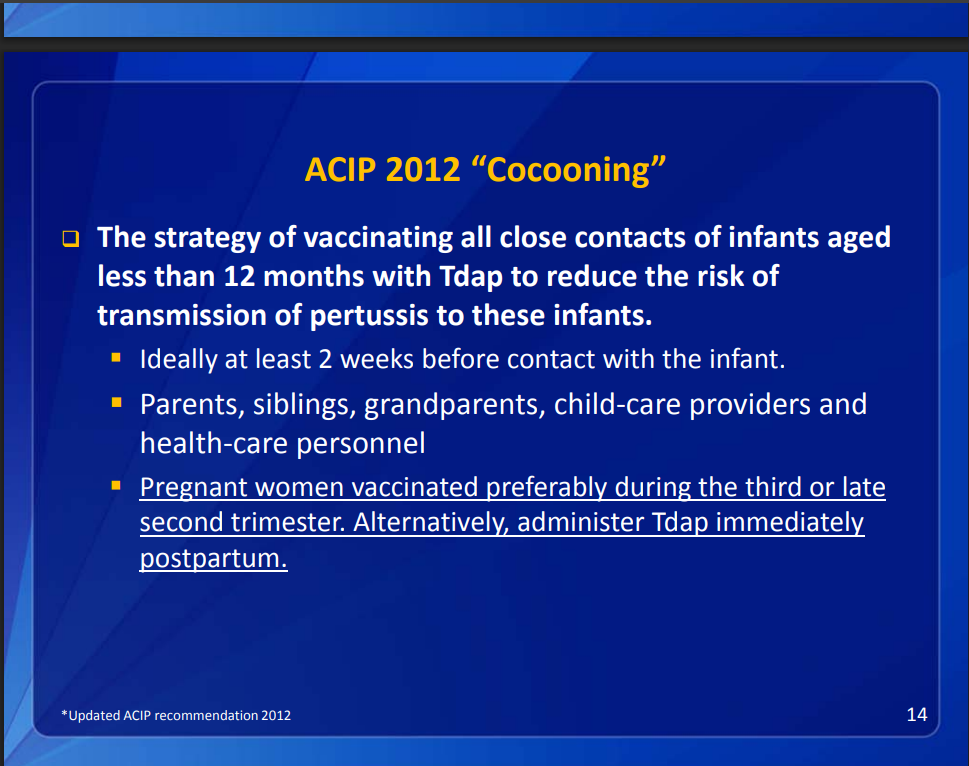
In 2005, ACIP recommended that close contacts of an infant be vaccinated at least 2 weeks before contact with the infant. Mothers were to be vaccinated right after birth.

Slide 9: Six years later, they concluded that cocooning did not work on a national level for a variety of reasons. Rather striking is the admission that they didn’t know if it was effective and had no system to measure coverage.

Slide 10: The recommendation shifted from vaccinating mothers postpartum to during pregnancy, supposedly to protect the infant. Yet, at the same time, they admitted they weren’t sure if maternal antibodies even prevent infant pertussis.

Despite recommending Tdap for pregnant women, the CDC openly acknowledges uncertainty about its effectiveness, as seen in Slide 11: "Concerns about Tdap in Pregnant Women."
It's only deemed “acceptably safe” by their data and experts.
They don’t know if maternal antibodies will actually prevent infant pertussis.
They worry it could weaken the infant’s immune response to the primary DTaP vaccine.
Yet, they believe the immediate—but uncertain—benefits outweigh the potential risk of reduced protection later.
In other words, they don’t know if it works but recommend it anyway.

However, ACIP, despite a lack of certainty that they were truly safe for pregnant women and effective for preventing pertussis in their offspring, went ahead with the recommendations, as slide 14 shows:
Could the Vaccinated Be Spreading Pertussis?
However, it may not be the unvaccinated who are responsible for infecting infants. Secondary vaccine failure and the inability of the vaccine to stop transmission are two reasons why it may be the vaccinated who are unwittingly spreading the bacteria and infecting infants.
The fact that the vaccine starts to wear off after children have received the last booster shot, so they may no longer be well protected, was highlighted by Children’s Health Defense in its coverage of the pertussis vaccine:
Numerous studies (both recent and not-so-recent) indicate that this dose-intensive vaccination regimen—far from providing meaningful protection—may actually be facilitating pertussis outbreaks.
Waning immunity (also called secondary vaccine failure) is one of the leading factors contributing to the pertussis fiasco.
A study published in 2013, the year after the recommendations were changed, showed that baboons that received the vaccine were protected from disease but were still colonizing and transmitting the bacteria once infected. CHD also spoke to the fact that the vaccine doesn’t protect others:
A number of studies have suggested that “vaccinated individuals may harbor and transmit [pertussis] infection, even in the absence of typical pertussis symptoms.” In a 2020 systematic review, the authors conclude that “the prevalence of asymptomatic infection is high” and that “frequent close contact occurring in household settings may provide sufficient opportunity for B. pertussis to spread.”
Unvaccinated individuals who contract pertussis will develop symptoms, so they will know to stay home until they recover. In contrast, vaccinated individuals can still transmit the virus, but since they are asymptomatic, they are not isolated and can unknowingly spread the illness. This suggests the pertussis vaccine could be counterproductive for most and a reason for the failure of the cocooning strategy.
CDC recommendations haven’t changed since 2012
Today, the CDC states that its evaluations and studies show that vaccinating mothers during pregnancy reduces infant pertussis, although it provides no outside confirmation of its conclusions. The agency recommends another vaccine for each pregnancy.
Health freedom requires engaged citizenship
The CDC’s playbook is clear: when a vaccine doesn’t work for the group that needs it most, the solution isn’t to rethink the approach—it’s to expand the campaign to those who don’t need it. This has occurred with flu, pertussis, and most recently, COVID-19. Rather than admitting failure, public health officials have pushed ahead, shifting the burden onto others while downplaying uncertainty and risks.
This pattern won’t change unless the public demands full transparency, independent oversight, and policies based on clear, measurable benefits, not assumptions or institutional inertia. With RFK Jr. now at the helm of HHS, there’s hope that it won’t be business as usual at the CDC. But real reform requires more than a leadership change—it requires an informed and engaged public unwilling to accept “this is CDC guidance” as an answer.
The information contained in this article is for educational and information purposes only and is not intended as health, medical, financial or legal advice. Always consult a physician, lawyer or other qualified professional regarding any questions you may have about a medical condition, health objectives or legal or financial issues.
I never thought I would say this. But we do need another vaccine. We need a vaccine that will give us guaranteed full immunity from the CDC. Now that’s one vaccine that I would stand in line to get. Except for the fact
that I already have full immunity since way before Covid started. Full immunity against the CDC virus. Thank God for small favors. Impossible for us , easy for Him!!!