



What You Haven't Been Told About Tetanus and the Tetanus Vaccine
'In spite of the ubiquity of the so-called cause, the incidence of tetanus is significantly low'


Disclaimer: The decision whether to have a tetanus shot should not be based solely on the information contained in this article. Parents and adults considering the shot for themselves should make this decision together with a trusted healthcare professional who provides information necesssary for informed consent — of the risks and benefits of both administering and not administering the shot.
What is Tetanus?
We've been told to fear tetanus with any wound, and hospitals will recommend a tetanus shot if you seek treatment. But, before you go ahead and roll up your sleeve, it’s important to have a better understanding of what tetanus is, its prevalence, and what the vaccine can and can’t do.
Tetanus is not a communicable disease or one that can be controlled through herd immunity. It is a poison produced by the spores of a bacterium that will only grow under anaerobic conditions. According to Immuniz.org,
Tetanus is caused by a toxin (poison) produced by the bacterium Clostridium tetani. The C. tetani bacteria cannot grow in the presence of oxygen. They produce spores that are very difficult to kill as they are resistant to heat and many chemical agents.
Stand for Health Freedom further explains that the spores can only produce toxin at temperatures between 35-37°C (95.666 – 98.6°F) or body temperature. It is the conditions that lead to the illness.
It is not the wound itself, nor the thing that caused the wound, that creates the illness. Your entire body could be coated in tetanus spores and you could still be free from tetanus infection. C. tetani bacterium are “obligate anaerobes,” meaning they will only reproduce in an environment without oxygen. The temperature range of 35-37 degrees Celsius (normal human body temperature) is the optimal temperature for reproduction, though it can reproduce to a lesser degree outside of that range. When the spores start reproducing to create new C. tetani, the process produces substances that are poisonous to humans and animals. The most dangerous is called “tetanospasmin,” which is the cause of what we know as tetanus. Tetanospasmin is a neurotoxin, meaning it is a poison to the nervous system.
Mortality and Morbidity
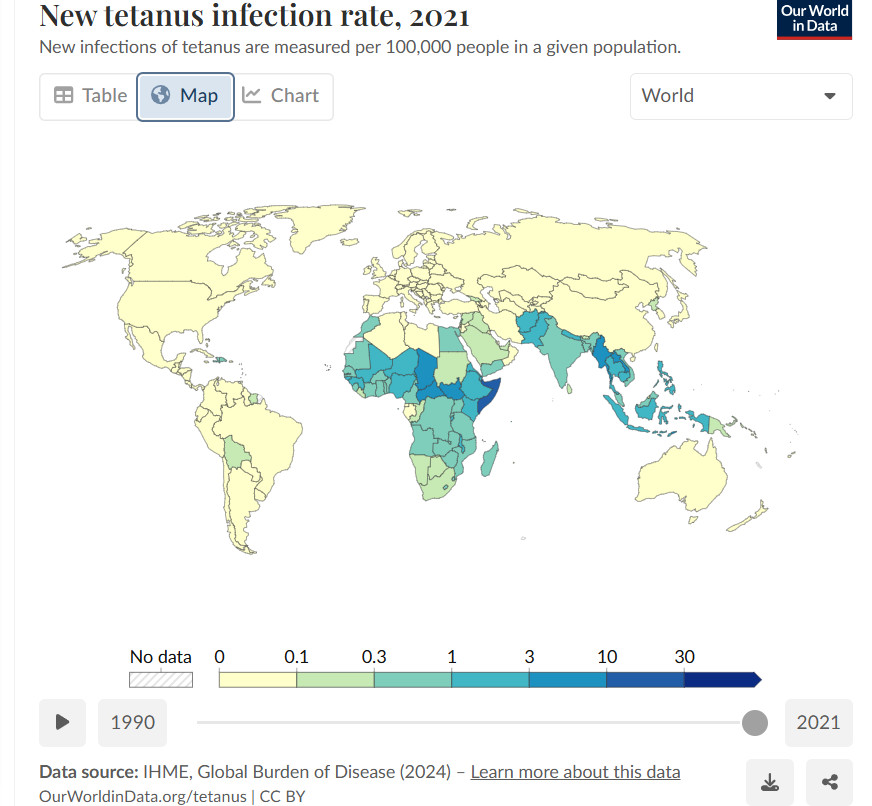
However, the chance of actually developing tetanus is another story. In the United States and most of the world, the disease is in decline. According to Our World in Data, tetanus cases are nearly nonexistent in the U.S. and much of the world, as shown in the map below.
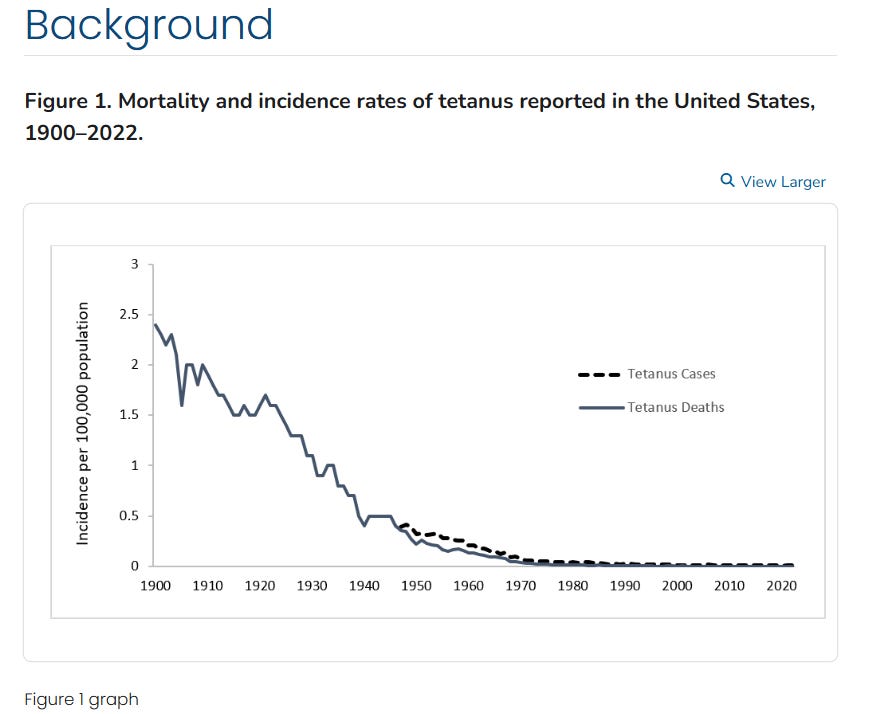
In the U.S., there were four recorded deaths from tetanus, predominantly in individuals 70 years or older, as illustrated in the graph below.

The CDC data shows that tetanus, like many childhood illnesses, was already decreasing in the early 20th century—even before vaccines were available.
Tetanus’s Decline
The CDC attributed the decrease post-1947 to the introduction of the vaccine and to the development of immune globulin prior to that, as well as better hygiene and wound care.
Next, the use of tetanus immune globulin (TIG), either for prophylaxis in wound management or for treatment of tetanus, has prevented cases and reduced the severity of tetanus cases. TIG first became available from equine sources during World War I in the 1910s, and then, human-derived TIG [much safer] became available in the 1960s. In addition, improved wound care, adoption of aseptic surgical techniques, and hygienic childbirth and wound care practices contributed to the decline in cases. Further, increased rural-to-urban migration with consequent decreased exposure to tetanus spores may also have contributed to the decline in tetanus mortality noted during the first half of the 20th century.
The CDC, in its Pink Book, noted that the vaccine introduced in the late 1940s targeted children.
In the late 1940s, tetanus toxoid-containing vaccines were introduced into routine childhood vaccination and tetanus became a nationally notifiable disease. At that time, between 500–600 cases (approximately 0.4 cases per 100,000 population) were reported per year.
Properly Treating Wounds
Stand for Health Freedom also explained that proper wound cleaning has remained the same for the past 100 years.
Wounds must be properly and thoroughly cleaned in order to mitigate tetanus infection. Stand for Health Freedom explains how this is done:
Standard treatment of a wound where tetanus is a possibility hasn’t changed in a century: The wound must be thoroughly and deeply cleaned, an injection of a serum to give the sick person antibodies can be given, and antibiotics are usually prescribed. The WHO recommends benzodiazepine drugs to reduce muscle spasms. In a nonmedical setting, some use homeopathic remedies like ledum and nux vomica or high doses of vitamin C to quell infection.
No matter whether people take medical or traditional approaches, the bottom line with staving off tetanus infections is always to get potential spores out of the wound as quickly and thoroughly as possible. This is why people will watch how much a wound bleeds as an indicator of the danger level for tetanus infection. Cleaning and “debriding” the wound —flushing and scraping out any foreign matter or dead skin — is essential for the best chance of stopping the spores from reproducing, releasing toxin, and attacking the nervous system.
Furthermore, as the Vaccine Information Network (VIN) notes, not every wound has the potential for tetanus. Not every wound contains tetanus bacteria, and tetanus bacteria have been isolated from patients who do not have tetanus. Tetanus spores, VIN explains, are ubiquitous, but few people are infected.
It is found on the surface of the body, in the mouth, in the gastro-intestinal tract, in house dust and clothing. It occurs extensively in cultivated soils. The organism lives as a harmless commensal in the gut of many animals, in addition to humans (rural residents tend to have higher rates of intestinal carriage than city dwellers). In spite of the ubiquity of the so-called cause, the incidence of tetanus is significantly low.
Medical literature going back to the 1920s has shown that, for the most part, c. tetani is innocuous, as VIN showed through the following examples.
In 1920, Sir Leonard Hill said in a report to the Medical Research Committee, “Tetanus and gas gangrene bacilli washed clean and injected are innocuous.”
In ‘A System of Bacteriology’ Vol III, page 307, Drs Bosanquet and Eyre say “The bacilli are in pure culture incapable of vegetating in viro,” ie of multiplying in the body.
In the Official History of the War, Pathology 1923, it is stated “Tetanus bacilli have been found in 20% of war wounds although no symptoms of tetanus were present, ” and “in 50% of undoubted tetanus cases the bacilli have been undiscoverable.” In the same volume also appears clostridium tetani has been “cultivated from the wound of a man showing no evidence of tetanus, 882 days after it had been inflicted,” and “it has been realised during the war that the tetanus bacillus or its spores may be present in vast numbers of wounds without producing tetanus.”
What About the Vaccine?
Immune.org explains that, if infected, it can take anywhere from 3 to 21 days for tetanus symptoms to appear.
The incubation period varies from 3–21 days, with an average of eight days. The further the injury site is from the central nervous system, the longer the incubation period. The shorter the incubation period, the higher the risk of death.
If tetanus is suspected, and someone isn’t up-to-date with their tetanus vaccinations, then the CDC recommends that immunoglobulin be given to provide immediate passive immunization. Complete protection is not said to occur until the entire series of tetanus shots is completed. It takes several weeks for antibodies to develop once vaccinated, according to Stand for Health Freedom:
In 1959, Drs. Donald Ross and J.J. Kraut co-authored a paper for “California Medicine” that noted, “To be effective, the course of toxoid inoculations must have been completed at least 30 days before the occurrence of the wound. Toxoid given at the time of injury to a patient who has not had a toxoid series of inoculations is without value. In no such circumstances can toxoid be a substitute for antitoxin.”
A 2016 study, “Durability of Vaccine-Induced Immunity Against Tetanus and Diphtheria Toxins: A Cross-sectional Analysis,” published in the journal Clinical Infectious Diseases, shows that if fully vaccinated, adults do not need boosters.
Mathematical models combining antibody magnitude and duration predict that 95% of the population will remain protected against tetanus and diphtheria for ≥30 years without requiring further booster vaccination.
VIN maintains that the vaccine is “pointless.” Proof is the decrease in neonatal tetanus in the developed world, well before antitoxins and vaccines came on the scene.
If we look at the documented Tetanus Mortality England & Wales from 1901 to 1999, we find that the administration of tetanus vaccine is likely to be pointless and puts children especially at risk of adverse reactions to the vaccines. (Link added.)
VIN also reports that unvaccinated populations have shown tetanus antibodies.
Debate as to whether humans can develop circulating antitoxin against tetanus in the absence of vaccination is futile since evidence of natural immunity has been observed globally.
Although there have been conflicting results, some studies in Brazil, China, Ethiopia, India, Italy, Israel, Spain and the USSR have shown substantial proportions of unimmunised populations with detectable levels of antitoxin. Specifically, up to 80% of persons in India and up to 95% of persons in a group of Ethiopian refugees had levels of antitoxin suggestive of protection. . . .
It is also known that an individual can get tetanus more than once. If there is no natural immunity produced, it is questionable how a vaccine can induce immunity. However, VIN states that ingesting the spores and their passage through the digestive system is how proper immunity is developed by natural means.
The development of tetanus by a deep puncture injury is known not to induce any subsequent immunity, which then raises the serious question — how is a vaccine able to produce any long-term immunity? Proper and natural immunity is achieved by the ingestion of tetanus spores through natural entry, stimulating the immune system at all levels in an appropriate way.
Researcher Vera Scheibner noted that injections are deep puncture wounds that bypass the “multi-leveled immune system,” the body's natural defenses. For the same reason, contracting tetanus through a puncture wound would not create proper immunity.
Critics of vaccination often highlight the fact that injecting foreign antigen into the body by-passes a branch of the immune system leading to a compromised host. Dr Viera Scheibner, a researcher on the ineffectiveness and dangers of vaccination, points out that any injection is a deep-puncture wound, so that is why contracting tetanus through a wound does not produce any long-term proper immunity because of the similar action to a vaccination, i.e. the by-passing of our multi-levelled immune system due to unnatural entry.
Dr. Cowen, writing for The Weston A. Price Foundation (WAPF), said that he had initially given the tetanus vaccine as the only vaccine to patients in his practice, believing that it was 100% effective per the National Institutes of Health (NIH).
. . . Thus, for a number of years, tetanus was the only vaccine I ever gave the children in my practice. I gave three shots, usually starting at about two years old and I never gave boosters. This was because of National Institutes of Health research, which claims that no one who has received all three shots for tetanus has contracted clinical tetanus.
However, subsequent information led him to rethink the vaccine. In addition to the drop in tetanus mortality even before the vaccines, it was revealed that the vaccine could make one susceptible to other infections.
[There have been some published studies showing that having tetanus antibodies facilitates the penetration of unrelated viruses into the cells. One of the viruses mentioned was HIV, another was hepatitis C. The implication is that somehow having tetanus antibodies from the tetanus vaccine makes one susceptible to seemingly unrelated viral infections. The mechanism of this is obscure and as far as I know there has been no follow-up. I can’t find this original reference, but I distinctly remember a patient showing me the research in the early 1990s. This, plus the worry about the chemicals used to preserve the vaccine, make this a more difficult choice than it was in the early days.
Reseau International claims that it is impossible for antibodies to prevent tetanus since it exists in areas where there is no blood or lymph, areas where the antibodies circulate.
Warning: it is not the bacillus itself that is dangerous for humans, but the toxin that it diffuses if it is in an anaerobic zone, for example a bruised wound with necrotic, non-vascularized flesh and crevices where precisely oxygen does not circulate given the absence of blood and lymph. This toxin, confined in the anaerobic zone, will be able to join the nerve endings which are in the wound and go up towards the central nervous system sheltered from the blood circulation, and it is there that it will be able to do damage. at the level of neuronal synapses by blocking the order of muscle relaxation.
Without going into the technical details of the mechanisms involved during the rise of the toxin in the nervous system, one thing is obvious: in the path taken by the tetanus toxin, there is no presence of possible antibodies since these are found only in blood and lymph. There is therefore no encounter between the toxin and the immune system in the natural course of the disease. How then can we claim that a vaccine, which generates antibodies, will be able to create immunity and therefore protect individuals from tetanus?
More troubling, however, is the finding that vaccinating for tetanus can cause a subacute form of tetanus that is not recognizable as such. Concerning, as well, is that a study found subacute tetanus can lead to gastrointestinal disturbances, responsible for causing increased gut permeability, learning delays, behavioral problems, and other issues as seen in autistic individuals.
The tetanus vaccine can give an atypical form of tetanus. The observations collected in Finland provide proof of this: “From 1969 to 1985, 106 cases of tetanus were declared in Finland; 66% of those affected were vaccinated. All those who had received at least the first three injections had an attenuated form which posed diagnostic problems. . . . All vaccines including tetanus toxoid are capable of causing the bastard forms of the disease they are supposed to prevent, with confusing symptoms and a disease state that is difficult to describe. Very often the doctors consider these pathologies as a harmless avatar of the vaccination and hardly worry about them. Yet the latent forms of a disease are often more worrying.
They reveal a very degraded ground and can be of a severe prognosis. The study conducted by Ellen BOLTE in the United States shows that children regularly vaccinated with routine vaccines, which include the tetanus vaccine, can develop "subacute" tetanus which can lead to significant disturbances in the intestine (in particular increased permeability) as well as behavioral disorders and stereotyped behaviors, learning delays, such as those developed in autistic people.
The Need for Independent Inquiry
The reality is that mainstream narratives often reduce complex issues to simple solutions—like a shot for every wound. But history, research, and even the medical literature show that the story isn’t that simple. Whether it’s the vaccine’s effectiveness, the role of natural immunity, or the risks that aren’t openly discussed, there’s more to the picture than we’re generally told. Making informed health decisions means looking beyond official recommendations, questioning assumptions, and weighing the evidence for yourself. After all, the responsibility for your health ultimately rests with you.
The information contained in this article is for educational and information purposes only and is not intended as health, medical, financial or legal advice. Always consult a physician, lawyer or other qualified professional regarding any questions you may have about a medical condition, health objectives or legal or financial issues.